|
Getting your Trinity Audio player ready... |
Dopamine Agonists Pharmacology in Parkinson’s Disease Treatment
Dopamine agonists are an important class of drugs used in the treatment of Parkinson’s disease (PD) and other related disorders, such as restless legs syndrome (RLS). This article provides an overview of their pharmacology, focusing particularly on their application in Parkinson’s disease. It explores their mechanism of action, common side effects, and potential drug interactions, while also addressing the clinical considerations and the role these drugs play in managing the disease.
Understanding Parkinson’s Disease Dopamine Agonists
Parkinson’s disease, first described by the British physician James Parkinson in 1817, is a progressive neurodegenerative disorder primarily characterized by motor symptoms. These symptoms include tremors (shakiness), muscle rigidity, bradykinesia (slowness of movement), and postural instability, which can significantly impair a person’s ability to perform daily tasks. As the disease advances, cognitive decline, dementia, and other non-motor symptoms, such as depression, anxiety, and sleep disturbances, may also occur.
The motor symptoms of PD arise from the degeneration of neurons in the substantia nigra, a region of the brain that plays a crucial role in controlling movement. These neurons produce dopamine, a neurotransmitter that is essential for the smooth and coordinated movement of muscles. When these neurons die, dopamine production is reduced, leading to the hallmark symptoms of Parkinson’s disease. Although the exact cause of neuronal death remains unclear, the accumulation of abnormal protein deposits called Lewy bodies is thought to contribute to the degeneration of dopaminergic cells in the brain.
Parkinson’s disease affects an estimated 6 million people worldwide, with a higher incidence among males and those with a family history of the disease. It typically manifests in individuals over the age of 60, though early-onset cases do occur. The disease progresses gradually, and while there is currently no cure, various therapeutic approaches, including medications like dopamine agonists, can help alleviate symptoms and improve quality of life.
Dopamine Agonists and Their Role in Parkinson’s Disease
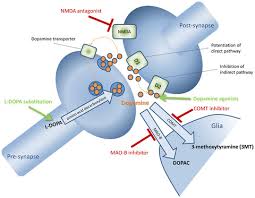
Dopamine agonists are one of the primary treatment options for Parkinson’s disease. These drugs mimic the effects of dopamine by binding to dopamine receptors in the brain, compensating for the reduced dopamine levels caused by neuronal degeneration. Unlike levodopa, another commonly used treatment, which is converted into dopamine in the brain, dopamine agonists directly stimulate dopamine receptors, providing symptomatic relief.
Several dopamine agonists are available for the treatment of Parkinson’s disease. Some of the most widely prescribed include:
- Ropinirole
- Pramipexole
- Cabergoline
- Rotigotine
- Bromocriptine
- Apomorphine
In addition to Parkinson’s disease, some of these drugs are also used to treat other conditions, such as restless legs syndrome (RLS), a disorder that causes an irresistible urge to move the legs, often accompanied by uncomfortable sensations.
Dopamine agonists are also used in the treatment of prolactinomas (tumors that produce excess prolactin) and acromegaly (a condition characterized by excessive growth hormone production), particularly cabergoline and bromocriptine.
Mechanism of Action
The underlying cause of Parkinson’s disease is a deficiency of dopamine in the nigrostriatal pathway, a part of the brain responsible for controlling motor function. Without sufficient dopamine, the basal ganglia (a group of nuclei in the brain involved in movement control) cannot effectively regulate motor movements, leading to the motor symptoms associated with the disease.
Dopamine agonists work by stimulating dopamine receptors, particularly the D2 receptor subtype, which is located in the basal ganglia. By activating these receptors, dopamine agonists help restore some of the motor control lost in Parkinson’s disease. These drugs have varying affinities for different dopamine receptors. For example, pramipexole has activity at the D2, D3, and D4 receptors, and its effects are thought to be more pronounced at the D3 receptor, which is associated with mood regulation and motor control.
Although dopamine agonists are effective in restoring dopamine function, they do not address the underlying cause of the disease—neuron degeneration—nor do they halt disease progression. Instead, these drugs serve as a means of managing symptoms and improving the patient’s quality of life.
Side Effects of Dopamine Agonists
While dopamine agonists can be highly effective in treating Parkinson’s disease, they are associated with a range of potential side effects. The most common side effects include:
- Nausea
- Drowsiness and dizziness
- Hallucinations and confusion
- Sleep disturbances
- Hypotension (low blood pressure)
- Muscle weakness
Apomorphine, in particular, is known to cause severe nausea and vomiting, and is often administered with an antiemetic to reduce these effects. Other dopamine agonists, like bromocriptine, also have emetic (vomit-inducing) properties but are less potent in this regard.
One of the more troubling side effects associated with dopamine agonists is the development of compulsive behaviors, such as gambling, hypersexuality, and overeating. This is believed to be due to the stimulation of dopamine receptors in areas of the brain involved in reward and motivation. Patients and their caregivers must be vigilant for these behaviors, as they can have significant personal and social consequences.
Other less common but still noteworthy side effects include peripheral edema (swelling in the legs and feet), constipation, and fatigue.
Clinical Considerations
The use of dopamine agonists requires careful consideration of several factors, particularly in elderly patients or those with pre-existing psychiatric conditions. These drugs can cause confusion and hallucinations, which may exacerbate underlying mental health issues. Consequently, caution is advised when prescribing dopamine agonists to individuals with a history of psychiatric disorders.
Dopamine agonists also pose a risk of hypotension, which can be particularly problematic in patients with cardiovascular disease. Patients should be monitored for signs of low blood pressure, especially when starting therapy or increasing the dose.
Another important clinical consideration is the potential for drug interactions. Dopamine agonists should not be used in combination with antipsychotic drugs or dopamine antagonists, such as metoclopramide, because these medications block dopamine receptors and can reduce the effectiveness of dopamine agonists.
Abrupt discontinuation of dopamine agonists is also contraindicated, as it can lead to withdrawal symptoms and, in rare cases, neuroleptic malignant syndrome (NMS), a potentially life-threatening condition. Gradual tapering is essential to avoid these complications.
For patients who cannot tolerate oral medications, transdermal patches, such as rotigotine, may be an alternative. These patches deliver the drug through the skin and provide a continuous, controlled release of the medication.
Conclusion
Dopamine agonists continue to be a cornerstone in the treatment of Parkinson’s disease, offering significant benefits in managing motor symptoms and improving the quality of life for patients. These medications work by mimicking the effects of dopamine in the brain, thereby compensating for the loss of dopaminergic neurons that characterizes the disease. While they are generally well tolerated, dopamine agonists can cause a range of side effects, including nausea, drowsiness, and compulsive behaviors. Careful monitoring and appropriate dose adjustments are crucial for minimizing these risks. Although they do not halt disease progression, dopamine agonists play a valuable role in the broader management strategy for Parkinson’s disease, which includes a combination of pharmacologic and non-pharmacologic treatments aimed at addressing both motor and non-motor symptoms.