|
Getting your Trinity Audio player ready... |
Beta-2 Agonists: Uses, Mechanisms, Side Effects, and Drug Interactions
Beta-2 agonists are a class of medications primarily utilized in the treatment of respiratory conditions such as asthma, chronic obstructive pulmonary disease (COPD), and hyperkalemia. These drugs are pivotal in the management of airway constriction and are employed to alleviate symptoms such as wheezing and shortness of breath. This article will explore the main beta-2 agonists used in clinical practice, the mechanisms through which they exert their therapeutic effects, potential side effects, and notable drug interactions.
Clinical Uses of Beta-2 Agonists
Beta-2 agonists are commonly prescribed for various conditions related to respiratory distress. These include asthma, COPD, and acute hyperkalemia, where they serve different therapeutic purposes based on their pharmacodynamic properties.
Asthma Treatment:
Asthma is a chronic inflammatory disease of the airways, characterized by intermittent episodes of wheezing, breathlessness, and coughing. Beta-2 agonists are particularly useful in managing these acute symptoms. Short-acting beta-2 agonists (SABAs) like albuterol (also known as salbutamol outside of the U.S.) provide quick relief by rapidly dilating the bronchial smooth muscle, easing the passage of air.
These medications are often used as “rescue” inhalers to be taken as needed during asthma attacks. On the other hand, long-acting beta-2 agonists (LABAs), such as salmeterol and formoterol, are utilized for long-term asthma management. However, LABAs are almost always combined with inhaled corticosteroids to reduce the risk of asthma-related complications and mortality, as monotherapy with LABAs has been linked to an increased risk of fatal asthma events.
Chronic Obstructive Pulmonary Disease (COPD):
COPD, a progressive lung disease commonly caused by smoking, involves persistent airflow limitation that can result in breathlessness and chronic cough. Beta-2 agonists are central in the treatment of COPD. SABAs like albuterol or terbutaline are used to relieve acute symptoms of shortness of breath during flare-ups. For maintenance therapy, LABAs such as salmeterol and formoterol may be prescribed. In severe cases, ultra-long-acting beta-2 agonists (ULABAs) like indacaterol and vilanterol are preferred for prolonged control of symptoms, given their extended duration of action.
Hyperkalemia:
Hyperkalemia refers to elevated potassium levels in the blood, which can lead to dangerous heart arrhythmias. Beta-2 agonists play a role in managing hyperkalemia in emergency settings. By stimulating the beta-2 receptors on cell membranes, these drugs promote the movement of potassium into cells, temporarily lowering blood potassium levels. Although beta-2 agonists are not a long-term solution for hyperkalemia, they are effective in acute scenarios as a bridge therapy until more definitive treatments can be administered.
Types of Beta-2 Agonists
Beta-2 agonists can be categorized based on the duration of their effects, which influences their clinical use. These include short-acting, long-acting, and ultra-long-acting agents.
- Short-Acting Beta-2 Agonists (SABAs):
- Examples: Albuterol (salbutamol), terbutaline.
- Use: SABAs are primarily used for quick relief of acute bronchoconstriction. They act within minutes and provide relief for several hours, making them ideal for use during asthma attacks or sudden exacerbations of COPD.
- Long-Acting Beta-2 Agonists (LABAs):
- Examples: Salmeterol, formoterol.
- Use: LABAs have a prolonged duration of action, typically lasting 12-24 hours. These agents are used for maintenance therapy in asthma and COPD, helping to prevent symptoms from occurring over the long term.
- Ultra-Long-Acting Beta-2 Agonists (ULABAs):
- Examples: Indacaterol, olodaterol, vilanterol.
- Use: ULABAs are characterized by an even longer duration of action, often lasting up to 24 hours. They are useful for patients who require consistent bronchodilation throughout the day and night.
The choice of which beta-2 agonist to use depends on the patient’s specific condition, the severity of symptoms, and the required duration of relief.
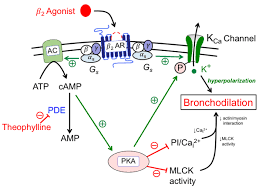
Mechanism of Action of Beta-2 Agonists
Beta-2 agonists exert their effects through the activation of beta-2 adrenergic receptors. These receptors are part of the sympathetic nervous system and are located in various tissues, including the bronchi, blood vessels, the gastrointestinal tract, and the uterus.
In the lungs, beta-2 agonists bind to these receptors, triggering a signaling cascade that ultimately results in the relaxation of bronchial smooth muscle. This bronchodilation facilitates improved airflow and reduces airway resistance, which is particularly beneficial during an asthma attack or COPD exacerbation.
Moreover, beta-2 agonists activate sodium-potassium ATPase pumps in the cell membranes, encouraging the movement of potassium from the extracellular space into cells. This action contributes to their therapeutic effect in hyperkalemia by lowering the concentration of potassium in the blood. However, this effect is short-lived and does not replace the need for more effective long-term treatment options for hyperkalemia.
Side Effects of Beta-2 Agonists
While beta-2 agonists are generally well-tolerated, they can cause a range of side effects, particularly at higher doses. Common side effects include:
- Palpitations and tachycardia: These are the result of the beta-2 agonist stimulating the heart’s beta receptors, which can lead to an increased heart rate.
- Hypokalemia: The potassium-lowering effect of beta-2 agonists can lead to a drop in blood potassium levels, especially when used in conjunction with other medications such as corticosteroids.
- Tremors and shakiness: These symptoms are a result of beta-2 receptor activation in skeletal muscle, leading to muscle tremors.
- Anxiety and restlessness: These central nervous system effects are often reported in patients using higher doses.
- Headache, insomnia, and hyperhidrosis (excessive sweating): These are other common side effects, often linked to the systemic effects of beta-2 agonists.
Serious, but rare, side effects may include arrhythmias, especially in patients with pre-existing cardiovascular conditions, and pulmonary edema.
Drug Interactions and Clinical Considerations
Certain drug interactions can influence the effectiveness or safety of beta-2 agonists. Notably:
- Beta-blockers: These medications may reduce the bronchodilatory effects of beta-2 agonists by blocking the beta-2 receptors. This can result in worsening bronchoconstriction, especially in asthma patients.
- Corticosteroids and theophylline: The combined use of beta-2 agonists with these drugs increases the risk of hypokalemia due to additive potassium-lowering effects.
- Cardiovascular considerations: Beta-2 agonists can induce tachycardia, so caution is warranted in patients with heart disease or arrhythmia risks. Long-term use, especially in high doses, can exacerbate underlying cardiovascular issues.
For optimal use, patients should receive thorough instruction on inhaler technique, as proper inhalation is critical for effective drug delivery. Healthcare providers should also regularly assess inhaler technique and the patient’s response to the prescribed therapy.
Conclusion
Beta-2 agonists are a cornerstone in the management of asthma, COPD, and hyperkalemia. By promoting bronchodilation and reducing blood potassium levels, these drugs provide critical relief during acute episodes. However, their use must be carefully managed to minimize side effects and drug interactions. As with all medications, patient education and regular monitoring are essential to ensure the best therapeutic outcomes and avoid complications.